Thoughts
Signals – quick single insights or data points
Notes – medium-length reflections
Longer in-depth essays

The Ring is the New Front Door
The front door to healthcare is a funnel: it directs patients to higher-level care, where the money is. Oura and Whoop are rebuilding that front door on a consumer subscription — and the demand it absorbs never shows up in the claims data.
AI Is Already Practicing Medicine
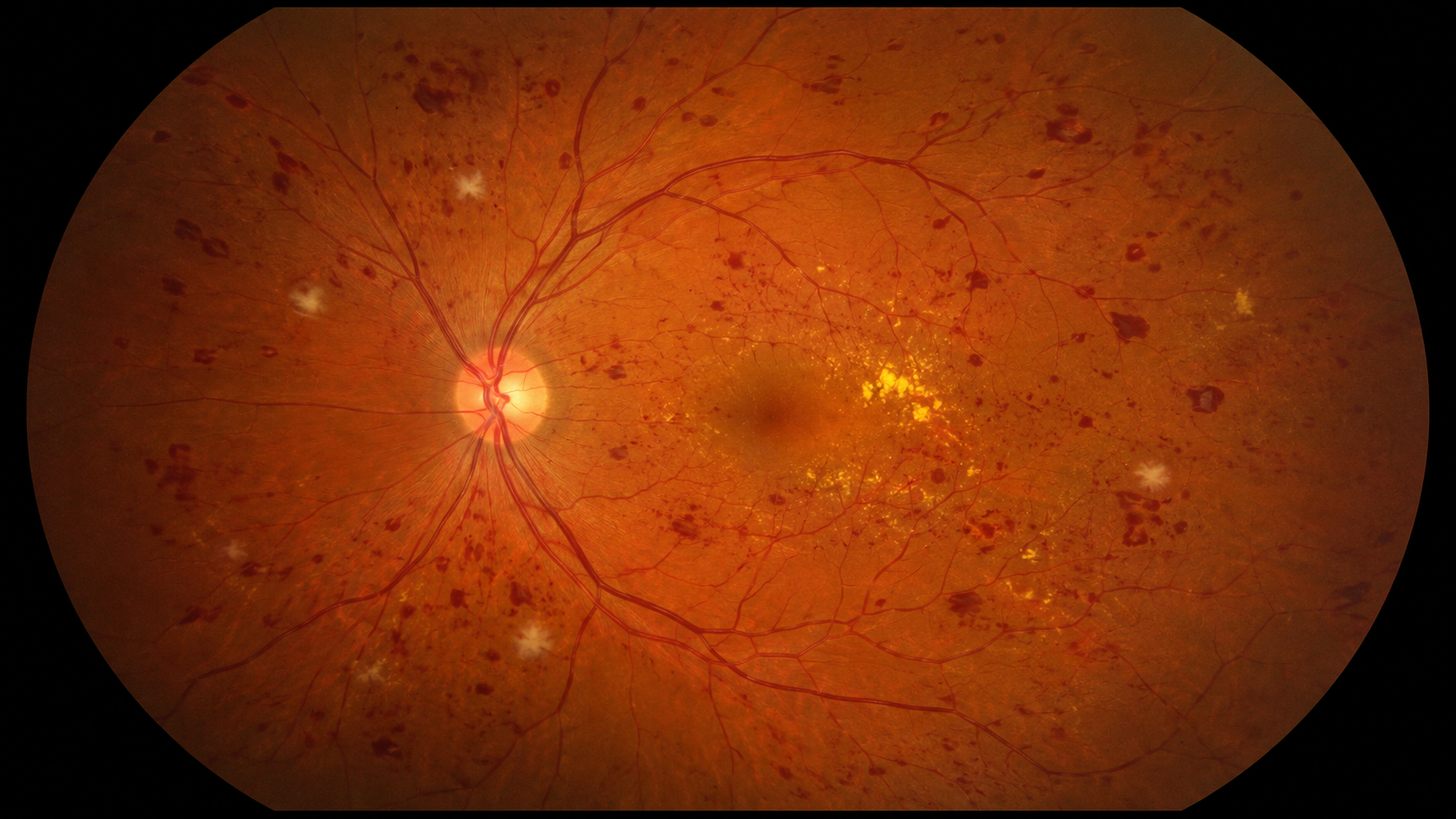
A surgeon posted on on LinkedIn that Silicon Valley, incorrectly, believes AI will be practicing medicine "momentarily." But AI has been diagnosing diabetic retinopathy with no physician since 2018, and this year another began renewing prescriptions in Utah. Both AI vendors carry malpractice insurance — because both AI systems are practicing medicine.
Correction re Fitbit Air: Apple Still Alone in Pricing Wearable AI Interpretation at Zero
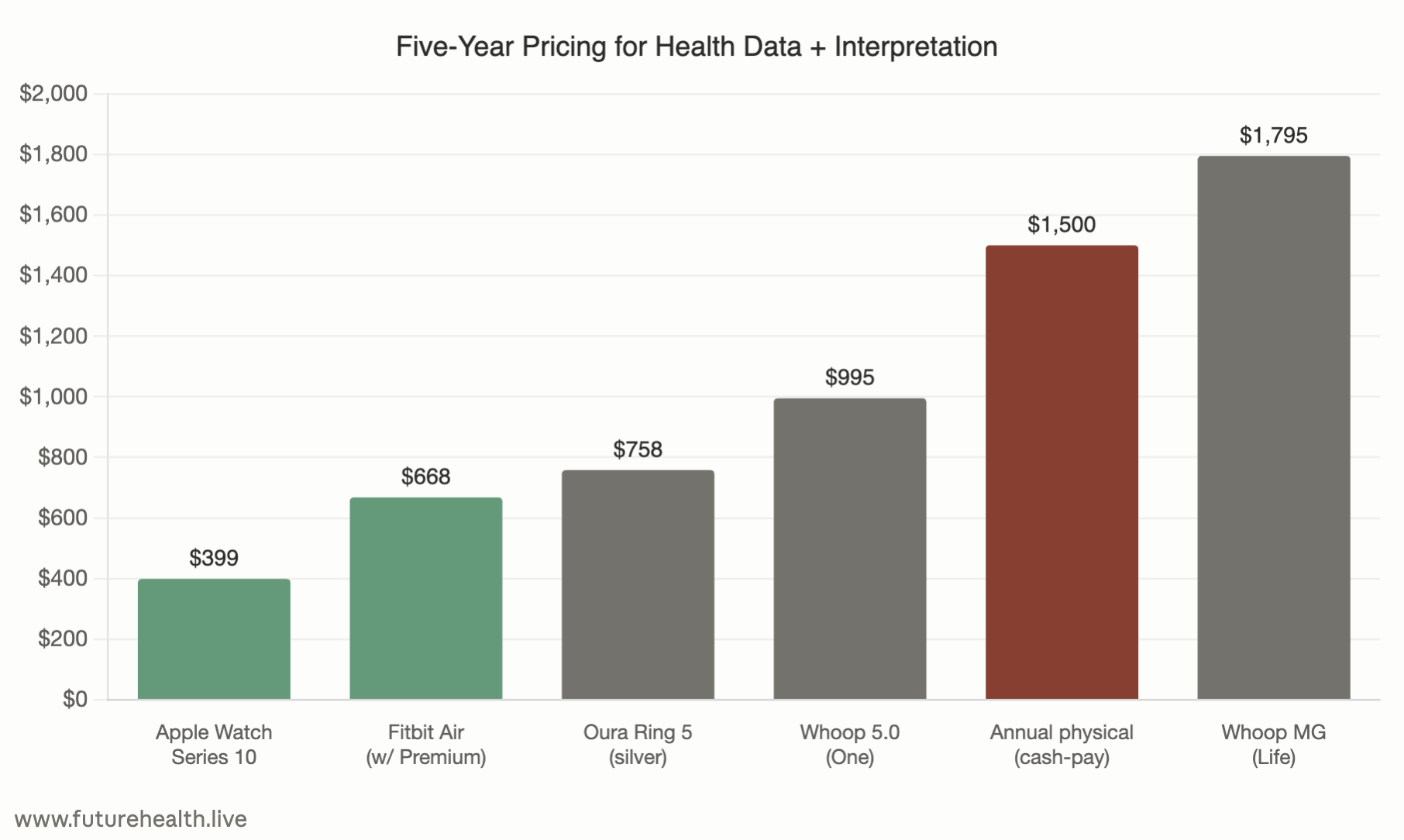
Correction to my previous post about the new Fitbit Air. Turns out Apple's Health app prices AI interpretation at zero — no subscription, ever. But the Fitbit Air doesn't. This leaves Apple in an unexpected position as the price leader for five years of hardware and AI interpretation — a full 40% less than Fitbit Air.

Signals: The Prescription Acne Drug You No Longer Need a Prescription For
A prescription acne combination just moved to the open drug store shelf — and the FDA's justification, not the drug, is the story. Treatment Migration continues.

Signals: Utah's AI Prescriber Was More Cautious Than the Doctors Auditing It
Five months into Utah's Doctronic pilot — the first US program authorizing AI to recommend prescription renewals — the state just released outcome data. The AI's renewal recommendations are statistically indistinguishable from a second physician's. And when the AI defers to a human, it defers more often than a human would.

AI Doesn't Replace Doctors. It Replaces the Reasons to See One
Danielle Ofri’s latest New York Times essay is the latest entry in a familiar genre: the physician explaining why AI cannot replace doctors. But the real question hospital systems, medical schools, and workforce planners need to answer is not whether AI will replace doctors. It is how many physicians we will need once the set of tasks that only physicians can perform are dramatically reduced.

Signals: Apple Found a Link Between Hearing and Mobility Just by Looking at Data From iPhones
For decades, hearing and exercise science depended on controlled studies conducted in clinics and universities, with specialized equipment and groups of volunteers. Now millions of people are generating real-world physiological and behavioral data every day through consumer devices — turning ordinary life into a continuous, global research platform.

Signals: Google Joins Apple in Pricing Health Interpretation at Zero
Apple has priced biometric interpretation at zero since 2015. Google joined them this week with the $99 Fitbit Air. Whoop and Oura now have to explain a five-year cost of ownership that runs seven to eighteen times higher — and the annual checkup has to explain why it still exists.

The Most Important Number Your Doctor Has Never Measured
There's a number that predicts whether you'll be alive in ten years better than your blood pressure, your cholesterol, your BMI, or whether you smoke. The American Heart Association has been recommending it as a vital sign since 2016. Your doctor has almost certainly never measured it. Apple Watch measures it every time you take a brisk walk.

Notes: 14 Million Appointments That Didn't Happen
Gallup says 14 million U.S. adults skipped a provider visit last month after using AI, which adds up to 168 million skipped visits per year. That's 16% of monthly physician visits — and it’s completely invisible in claims data, and ignored in healthcare planning.

Signals: AI is Killing 14 Million Clinic Visits — Per Month
Gallup and West Health just gave us some solid data on demand migration.
In a nationally representative survey of 5,500 U.S. adults released April 15, 14% said the AI-generated advice led them to skip a provider visit in the past 30 days. Projected to the adult population, that's roughly 14 million missed appointments in a single month.
Notes: the Prescription You Can’t See
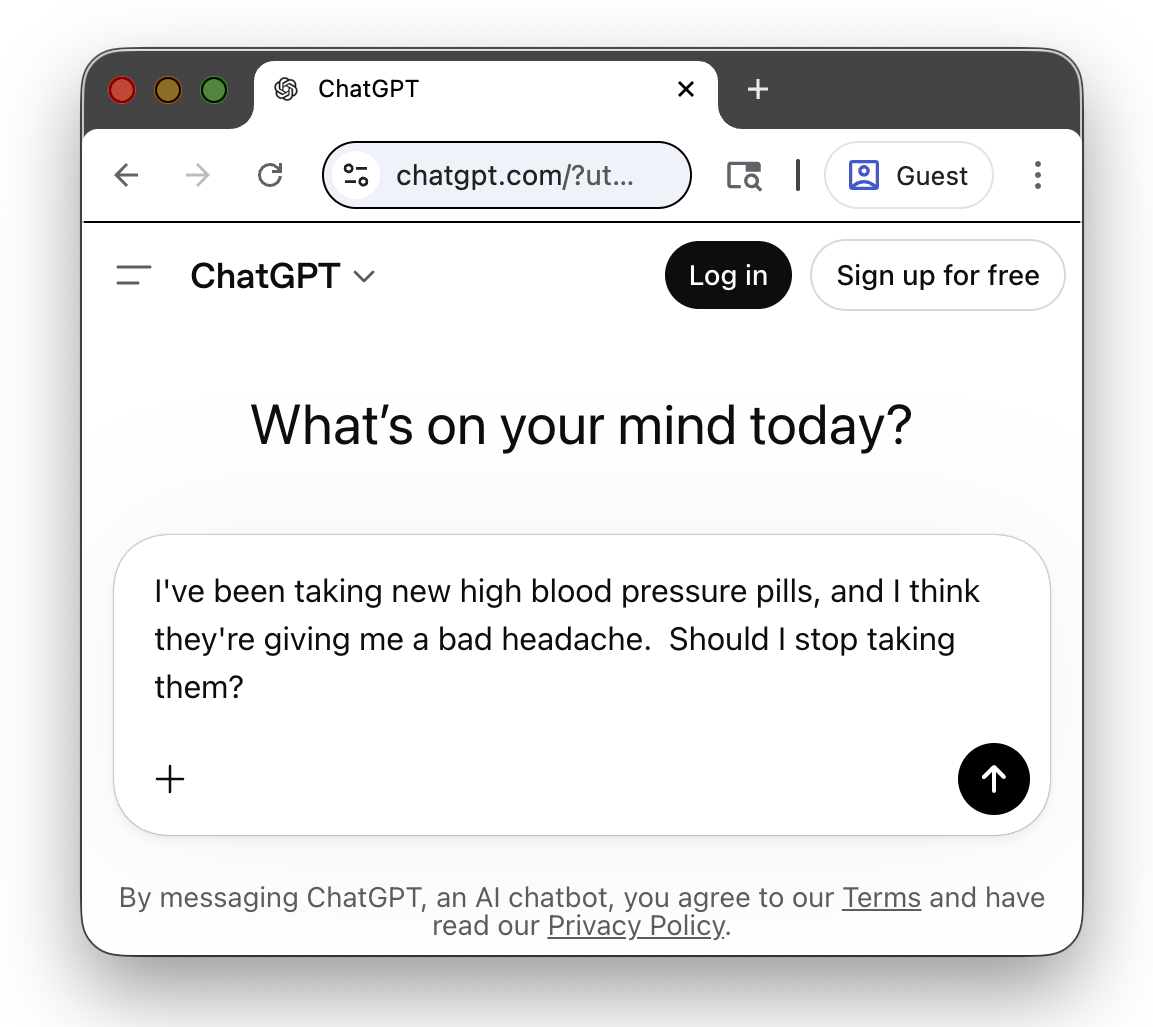
Eighteen percent of AI chatbot users have adjusted a medication based on a chatbot conversation. No doctor, no clinical oversight, no documentation anywhere in the healthcare system. The prescribed regimen and the actual regimen are diverging moore and more, via a channel that is invisible to healthcare.
The $50B Measurement Blind Spot in Healthcare Strategy
I speak with at least 100 healthcare leaders each year. They track everything — length of stay, readmissions, OR utilization, revenue cycle velocity. The one thing they're not tracking at all? The demand leaving the system entirely. And a Harvard finding that should have set off alarms six years ago has gone almost completely unnoticed.

A Podcast with Scott Becker of Becker’s Hospital Review
Happy to discuss healthcare growth, primary care’s decline, consumer health tech, and self-driving cars with the very well-informed Scott Becker, in this episode of Becker’s Healthcare Podcast.
The ATM, the iPhone, and Your Doctor's Office
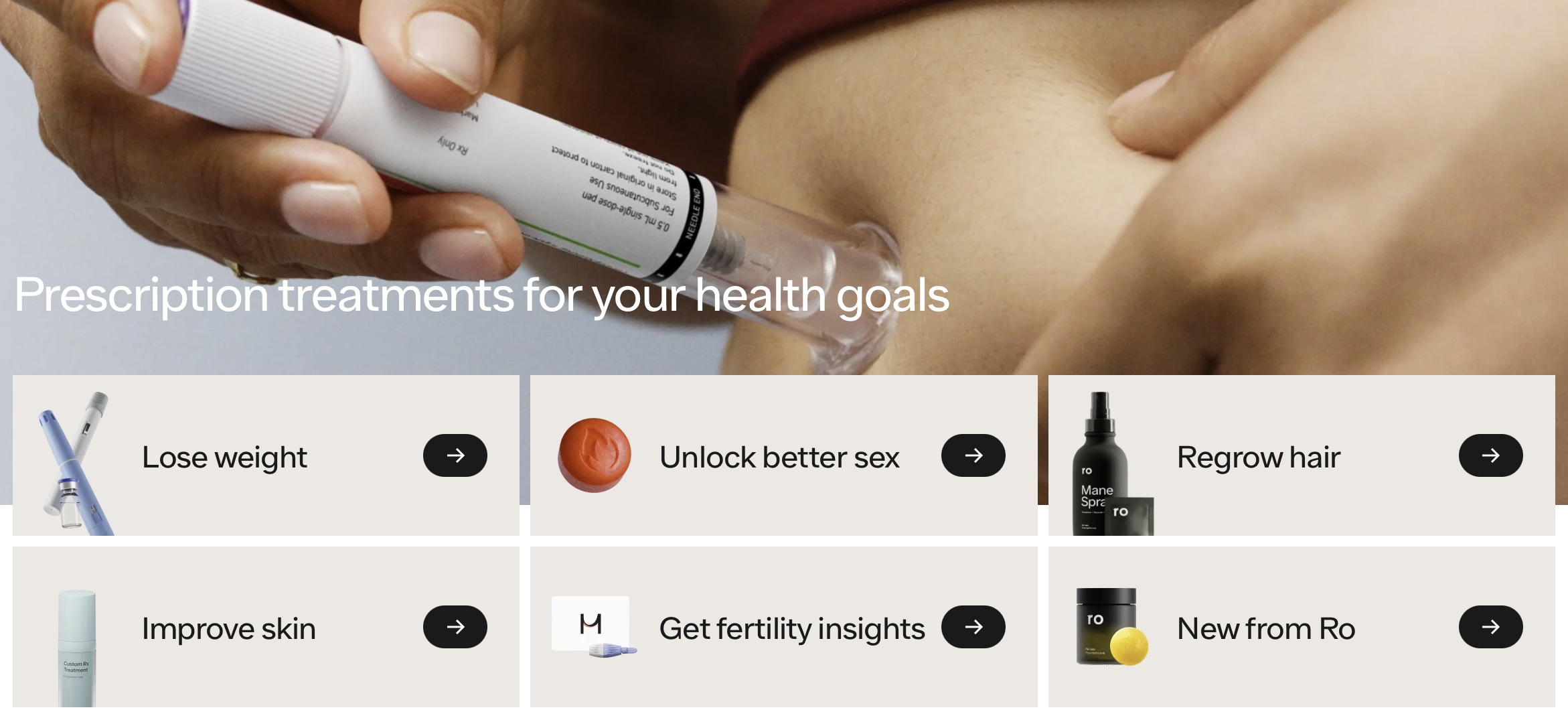
Clinical AI can make doctors more efficient and reduce burnout. But wearables, GLP-1 drugs, direct-to-consumer labs, and AI health assistants are doing something far more radical: they’re making many traditional doctor visits unnecessary. The real disruption in healthcare is already happening outside the exam room.
Signals: Was the Diagnosis Already in the Chart?
Stanford researchers gave AI radiology test questions without the images. The AI aced them anyway. Most people think that's a knock against AI. I think it's telling us something about the images.

Signals: Geoff Hinton Not Wrong After All?
Hospital CEOs are saying they’re ready to replace radiologists with AI for first reads. The radiology community has spent nine years saying that would never happen.
They can’t both be right.
Your Doctor’s Favorite AI Has Never Been Tested
40% of U.S. physicians use OpenEvidence. DoxGPT had 300,000 clinician users last quarter. UpToDate just launched Expert AI. Not one of these tools appears to have been independently tested for accuracy or safety. A profession built on evidence-based medicine is adopting AI with no evidence.
The Economist Wrote About Healthcare Disruption — But Missed the Disruption
The Economist says healthcare has "proved resistant to treatment from disrupters." If that's true, why has per capita spending growth been falling for fifty years? Why have primary care visits dropped 24%?
Because the Economist, and the healthcare system, don't count disruption that doesn't call itself healthcare.
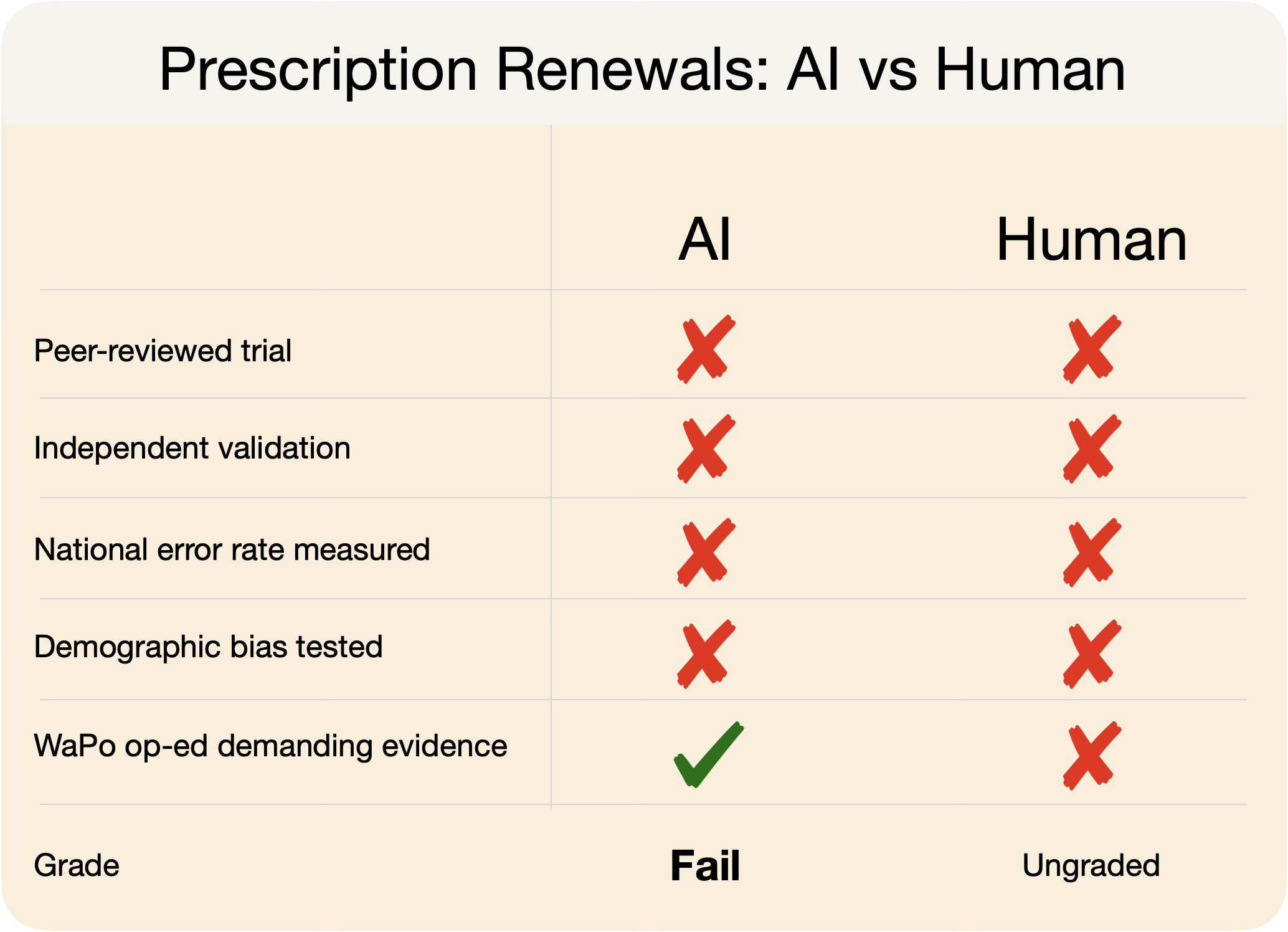
We Want to Grade the AI. Did We Grade the Doctor?
A Washington Post op-ed argues that Utah's AI prescription renewal pilot rests on thin evidence. Fair. But the human renewal process it's replacing has never been rigorously validated either. We're applying a standard to AI that we've never applied to the human baseline.