Thoughts
Signals – quick single insights or data points
Notes – medium-length reflections
Longer in-depth essays

The Ring is the New Front Door
The front door to healthcare is a funnel: it directs patients to higher-level care, where the money is. Oura and Whoop are rebuilding that front door on a consumer subscription — and the demand it absorbs never shows up in the claims data.

AI Doesn't Replace Doctors. It Replaces the Reasons to See One
Danielle Ofri’s latest New York Times essay is the latest entry in a familiar genre: the physician explaining why AI cannot replace doctors. But the real question hospital systems, medical schools, and workforce planners need to answer is not whether AI will replace doctors. It is how many physicians we will need once the set of tasks that only physicians can perform are dramatically reduced.

The Most Important Number Your Doctor Has Never Measured
There's a number that predicts whether you'll be alive in ten years better than your blood pressure, your cholesterol, your BMI, or whether you smoke. The American Heart Association has been recommending it as a vital sign since 2016. Your doctor has almost certainly never measured it. Apple Watch measures it every time you take a brisk walk.

Notes: 14 Million Appointments That Didn't Happen
Gallup says 14 million U.S. adults skipped a provider visit last month after using AI, which adds up to 168 million skipped visits per year. That's 16% of monthly physician visits — and it’s completely invisible in claims data, and ignored in healthcare planning.
The $50B Measurement Blind Spot in Healthcare Strategy
I speak with at least 100 healthcare leaders each year. They track everything — length of stay, readmissions, OR utilization, revenue cycle velocity. The one thing they're not tracking at all? The demand leaving the system entirely. And a Harvard finding that should have set off alarms six years ago has gone almost completely unnoticed.
When Enterprise Health AI Makes a Mistake, Who’s Liable?
Medicine has a well-established model for distributing liability across physicians and tools: whoever caused the failure bears the liability. AI vendors have quietly opted out of it — and the contracts they're asking health systems to sign reflect that.
When Consumer Health AI Makes a Mistake, Who's Liable?
In the first week of January 2026, Utah, and OpenAI each drew a different line around health AI—and liability. Utah’s Doctronic pilot treats AI like a clinician, with malpractice coverage and preserved remedies. OpenAI adds medical-record syncing under unchanged disclaimers and a $100 cap.

The Continuous "Dr. You": OpenClaw and the Future of Personal Health Management
Current AI health tools share the same flaw as traditional healthcare: they're episodic, not continuous. OpenClaw — a nerdy new tool that’s shot to 2 million users in nothing flat — shows us what comes next: AI assistants that monitor your health 24/7, cross-reference data sources, and act on your behalf without being asked.
From Exam Room to Living Room: The New Health System, Part 1
For the last 50 years, the engine of technology innovation has been a consumer engine. Consumers have steadily accumulated new health capabilities—including diagnosis, treatment, and monitoring—much faster than healthcare organizations. This has caused a decades-old, large-scale migration of health-related activity from the healthcare system to the consumer tech system. But in my experience speaking with hundreds of healthcare CEOs and board members, these migrations remain largely invisible to healthcare leadership.

Digital Coaches, Part III: FDA + Utah Accelerating the Consumer Health Shift
The FDA just updated its General Wellness guidance, allowing consumer devices to measure clinical parameters for coaching—no clearance required. The same week, Utah let AI renew prescriptions with no doctor. Both are doing the same thing: moving healthcare tasks out of traditional systems and into consumer channels.

The New York Times Got Smaller — Healthcare Is Next
The New York Times built one of the best digital products in media—yet its real revenue and profit have fallen by more than half. That’s what disruption actually looks like: the work moves elsewhere while the industry shrinks. Healthcare is now entering the same pattern, driven by consumer tech, GLP-1s, and safer mobility. We’re heading toward better health—and a smaller healthcare system.

Digital Coaches, Part II: Prevention’s New Business Model
Digital coaches are taking prevention where healthcare and public health can’t reach — into daily life. Activity trackers like Apple Watch, Fitbit, and Garmin now deliver personalized, continuous feedback at global scale, turning prevention into a business that keeps people healthier — and needing healthcare less.

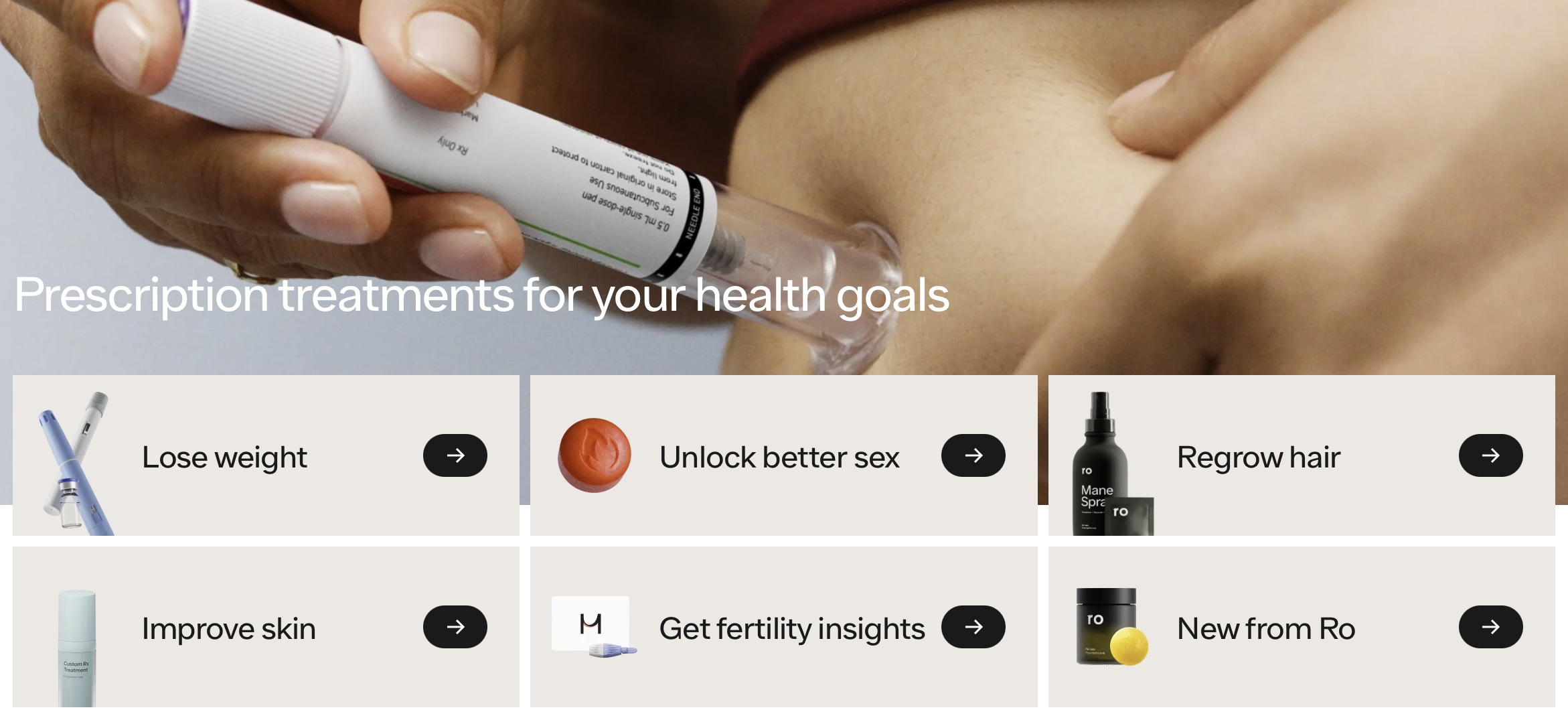
The Rise of Digital Health Coaches
AI health coaches aren’t just for athletes anymore. They’re starting to handle the day-to-day interpretation, advice, and treatment adjustments that once required doctors. From glucose monitoring to hypertension management, technologies like Dexcom, Teladoc, and Omada are quietly taking over the work of routine clinical decision-making. This new generation of digital health coaches marks the next step in a long trend — technology shrinking healthcare by making us need it less.

Hidden Connections: What John Muir Can Teach Us About Apple’s New Hypertension Notifications
The naturalist John Muir saw how everything in nature is connected — and today AI is showing us the same truth inside the body. From Apple Watch studies on atrial fibrillation to new hypertension alerts, hidden links in long-collected data are transforming how we understand health.

Forget the EHR — Your Health Data’s On Your Phone
The overwhelming majority of health-relevant data —movement, behavior, speech, sleep — is now generated outside the clinical setting. As a result, health innovation is increasingly shifting toward consumer devices and tech platforms that actually hold the data — not the EHR or the healthcare system.

Is Autonomous Driving Healthcare’s Most Important Competitor?
Hospitals worry about retail clinics and other healthcare competitors. But real disruption may come from outside healthcare entirely: cars that don’t crash. As autonomous driving becomes safer and more widespread, the revenue ripple effects on emergency departments, orthopedics, and imaging will be profound—and sooner than most systems expect.

The Empowerment of Consumers for Health: A Long Trend, Accelerated by AI
The public conversation about AI in healthcare swings between extremes—some predict it will replace doctors, others that it will usher in a golden age for medicine. So which is it? In my recent American Family Physician editorial, I explore how AI is less a disruptor of doctors than a powerful accelerator of consumer-driven health.

The Coming Collapse of Medical Demand
Innovations like GLP-1 drugs, self-driving cars and AI therapy chatbots are driving down illness, injury and the demand for traditional care. Rather than just improving delivery, these shifts reduce the need for doctors altogether. Snack food CEOs are planning for an Ozempic world. Why aren’t healthcare execs?

Disruption for Doctors 2: Healthcare Examples
Smartphone apps that can diagnose pneumonia? FDA-approved machines that can diagnose conditions without a doctor? Robot psychotherapy? It’s not coming, it’s here now.