The Economist Wrote About Healthcare Disruption — But Missed the Disruption
The Economist published a piece earlier this month profiling what it calls "a new wave of disrupters" taking on American healthcare — from DTC prescription platforms to AI chatbots to venture-backed diagnostic startups — as digital health attracted $14 billion in VC funding in 2025, up 35% from the year before.
The article's central premise goes like this: American healthcare has "proved resistant to treatment from disrupters." Google tried and failed. IBM tried and failed. Amazon tried and failed. But now — with AI improving, patients fed up, and regulators loosening — maybe this new wave will finally break through.
That premise is wrong. Not the part about the new wave — those companies are real, and some of them will matter. The part that's wrong is the claim that past disruption failed. It didn't fail. It succeeded — massively, over decades — and the healthcare system (and the Economist) never noticed, because the disruption happened outside the walls, and no one was measuring.
Decades of disruption, ignored
The Economist lists Google as its first example of a failed disrupter. In 2008, Google launched a platform to help people store and manage their health records. It shut down in 2011 after failing to gain users.
Google: all-time healthcare disruption champ
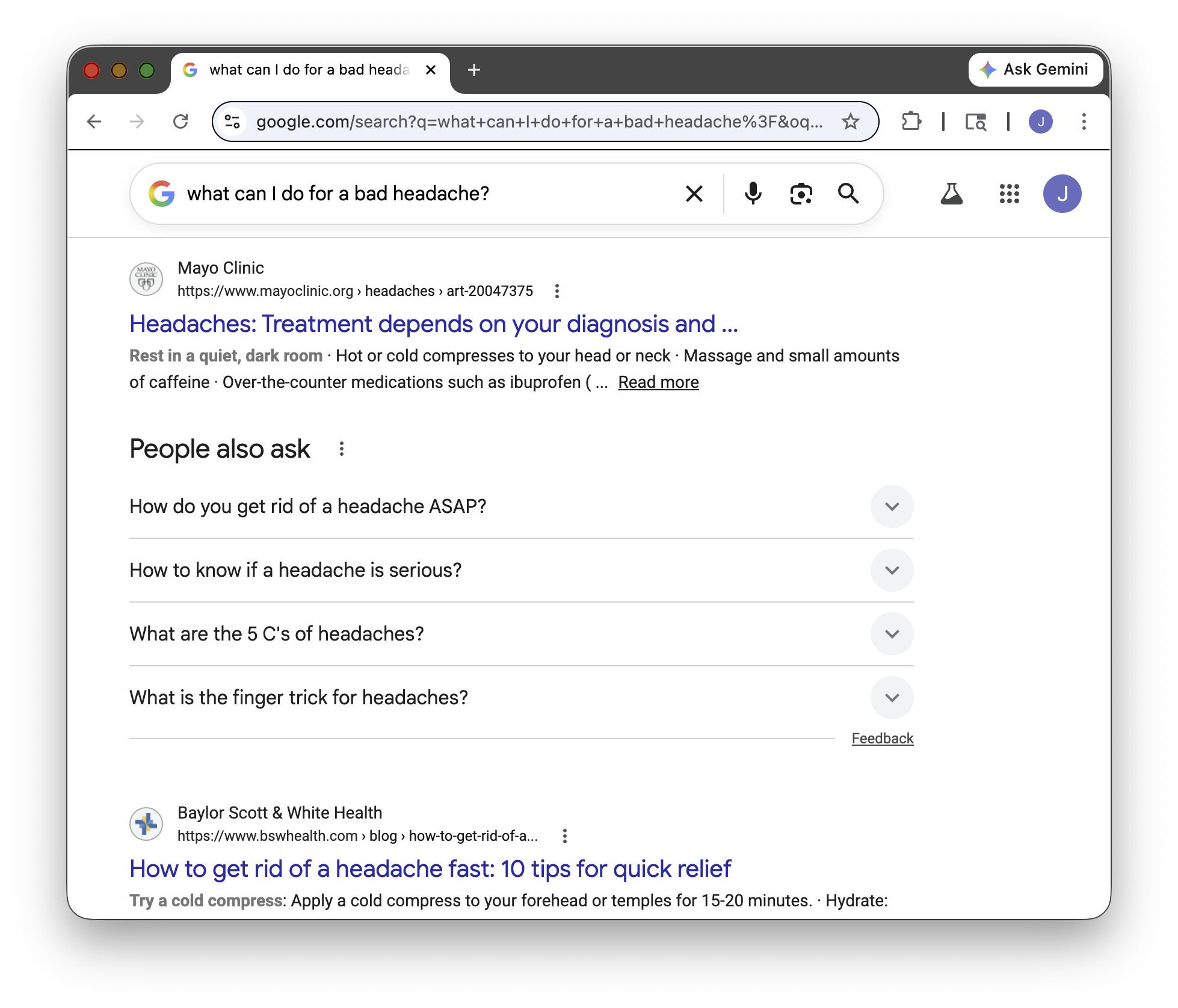
Fair enough. Google Health the product was a flop. But Google Search has been arguably the most successful healthcare disrupter in history. How many people have Googled a symptom over the past twenty years and decided they didn't need a doctor? How many sore throats, rashes, back pains, and anxious late-night questions were resolved — well or poorly — by a search engine instead of a physician?
No one knows. Because the healthcare system only measures health activity that happens in clinics, or wears a white coat. Google Search didn't show up in any claims database or utilization report. It generated no encounters, no referrals, no billing codes. So the industry filed Google under "failed disrupter" and moved on — while the actual disruption continued at a scale no startup has come close to matching.
Google isn't even the oldest example. The disruption started in the pharmacy aisle. Every time the FDA switches a drug from prescription to over-the-counter — Prilosec, Claritin, Flonase, Plan B, Narcan — a healthcare task migrates from the exam room to the consumer. The patient who once needed an appointment, a copay, a provider, and a prescription now walks into CVS and handles it themselves. That visit disappears from the system. No claim is filed. No encounter is recorded.
OTC switches have been happening for decades. They are explicitly designed to remove doctors from the equation, and that is what they have been doing, very effectively. Nobody calls them disruption. But they are, and one of the most effective forms of it — just invisible to the institutions losing the volume.
The Data Shows Healthcare Has Been Shrinking for Years
If past disruption really failed — if healthcare truly "proved resistant" — you'd expect the data to show a system holding steady or growing. It shows the opposite.
Real per capita healthcare spending growth in the United States has been falling for half a century (per CMS data). In the 1960s, per capita expenditure (in 2023 dollars) grew 83% over the previous decade. By the 1980s: 51%. The 2000s: 30%. The most recent decade: 28%. And since 2000, real per capita spending has actually declined in absolute terms multiple times — something that has never happened before in the 60+ years or so we've been keeping track.
The Economist opens with a striking number: America spends $5 trillion a year on healthcare. That figure is meant to convey the enormity of the fortress. But on a per-person, inflation-adjusted basis, the fortress has been losing ground for decades, and has outright contracted in several recent years. Something has been siphoning demand out of the system for a long time. Whatever that is, healthcare doesn't look like a system that "proved resistant to treatment from disrupters."
Then there are the visits. A 2021 study by Ganguli and colleagues in JAMA Internal Medicine found that primary care visits in the United States fell 24% between 2008 and 2016. Twenty-four percent! And three-quarters of that decline couldn't be accounted for by any shift visible in claims data — no transfer to urgent care, no movement to telehealth, no substitution by specialists. The visits just vanished — though the study authors suggested that a large portion could be attributed to former patients, especially "younger, healthier adults, who may have fewer routine care needs and be increasingly comfortable with online self-care."
Slowing spending growth. Absolute spending declines. A quarter of primary care visits gone with no trace in claims data. Decades of OTC switches moving treatment tasks to pharmacy aisles. Billions of health queries answered by Google.
This isn't a system that resisted disruption. This is a system that was disrupted and didn't notice.
The New Wave Is Real — and It Fits the Pattern
The Economist is right that something new is happening. But the new companies aren't breaking through a wall that previous disrupters couldn't breach. They're accelerating migrations that have been under way for a generation.
I've been writing about this as the Five Migrations — the systematic movement of healthcare tasks from clinical settings to consumers. Knowledge. Diagnosis. Treatment. Monitoring. Interpretation. Each follows the same arc: a task that once required a clinician in a clinical setting becomes something a patient can do themselves.
The Economist's company catalog maps directly onto this framework:
Knowledge and Interpretation. OpenAI says more than a quarter of ChatGPT's 900 million weekly users ask at least one health question — most outside clinic hours. This is the Knowledge Migration that started with Google Search, now turbocharged by AI that can hold context, interpret lab results, and personalize. ChatGPT didn't create the demand. It's serving demand that has been migrating away from clinicians for twenty years.
Treatment. Hims & Hers and Ro started with hair loss and erectile dysfunction — low-stakes categories that most physicians barely contested. Now they sell GLP-1 prescriptions for weight loss, one of the most medically significant treatment categories in a generation. That's the classic Christensen pattern: disrupters enter at the bottom of the market, where incumbents don't bother to compete, then move upmarket. Drugmakers are already responding by selling directly to consumers. Every one of these transactions is a visit that didn't happen — the same Treatment Migration that OTC switches have been driving for decades, now extending into categories that matter enormously to the traditional system.
Diagnosis and Monitoring. Prenuvo sells full-body MRI scans for around $1,000. Function Health sells comprehensive blood panels for periodic monitoring. These look new, but the Diagnosis Migration started decades ago — with the home pregnancy test. Then came home HIV tests, home strep tests, home COVID tests. Each one moved a diagnostic task from a clinician's hands to a consumer's. The Monitoring Migration followed the same path: the home blood pressure cuff, the home glucose monitor, Fitbit, Apple Watch, continuous glucose monitors now worn by people without diabetes. Prenuvo and Function Health are the latest step, not the first. And like their predecessors, they're largely serving demand the clinical system ignored — because guidelines didn't call for screening, or because the patient never made it to the appointment where the conversation would have happened.
The Gatekeeper Objection
The article surfaces the standard physician rebuttal: consumer-purchased scans and tests will flag benign conditions and strain an already stretched system.
This is the exact argument incumbents make at every stage of a Christensen disruption. The new product is inferior. It creates waste. It serves people who don't really need it. Minicomputers were toys. Online brokerages were for amateurs. Nurse practitioners shouldn't practice independently.
The pattern: gatekeepers define what counts as necessary, then object when consumers make a different assessment. But the consumer who pays $1,000 for a Prenuvo MRI has decided the information has value to them — regardless of whether a physician would have ordered it.
And most of these companies aren't competing with doctors. They're competing with nothing — which is what many people were getting before. When a third of American adults are skipping or delaying care because of cost, doing nothing ("nonconsumption" in Christensen terms) is the real alternative. The startups are competing, and winning, against that.
What you can’t see CAN hurt you
The Economist concludes that American healthcare "may not be immune to change for much longer."
That gets the tense wrong.
Per capita spending growth has been falling for fifty years. Real per capita spending has declined outright, multiple times, since 2000. Primary care visits dropped 24% before Hims existed. Billions of health questions were answered by Google before ChatGPT launched. OTC switches have been migrating treatment tasks out of the exam room for generations.
The reason the Economist — and most of the healthcare industry — keeps missing this is structural. The system measures what happens inside its walls. Claims data. Encounter records. Utilization reports. These instruments are precise, comprehensive, and blind to the most important trend in healthcare: the growing share of care that happens outside the system entirely. The spending data confirms it. The visit data confirms it. The companies the Economist profiles confirm it.
So The Economist noticed the disruption of the last three years — it just missed the last three decades.
Previously: We Want to Grade the AI. Did We Grade the Doctor?
Coming next: Your Doctor's Favorite AI Has Never Been Tested